
Fungal peritonitis isn’t common, but when it happens, it’s dangerous. It mostly affects people on peritoneal dialysis, those who’ve had abdominal surgery, or patients with weakened immune systems. Left untreated, it can lead to sepsis or death. That’s where voriconazole comes in - one of the few antifungal drugs that actually works against the fungi causing this infection.
What Is Fungal Peritonitis?
Fungal peritonitis is an infection of the peritoneum - the lining of the abdominal cavity. Unlike bacterial peritonitis, which often comes from a ruptured appendix or bowel, fungal cases usually start from fungi entering the peritoneal space through a catheter, surgical site, or from the bloodstream. The most common culprits are Candida species, especially Candida albicans, but Aspergillus and other molds can also cause it.
Patients on long-term peritoneal dialysis are at the highest risk. Every time they connect or disconnect their dialysis bags, there’s a chance for contamination. Antibiotics used to treat bacterial infections can wipe out good bacteria and let fungi take over. Studies from the European Dialysis and Transplant Association show that fungal peritonitis accounts for about 5% of all peritonitis cases in dialysis patients, but it’s responsible for over 20% of treatment failures.
Why Voriconazole? The Science Behind the Choice
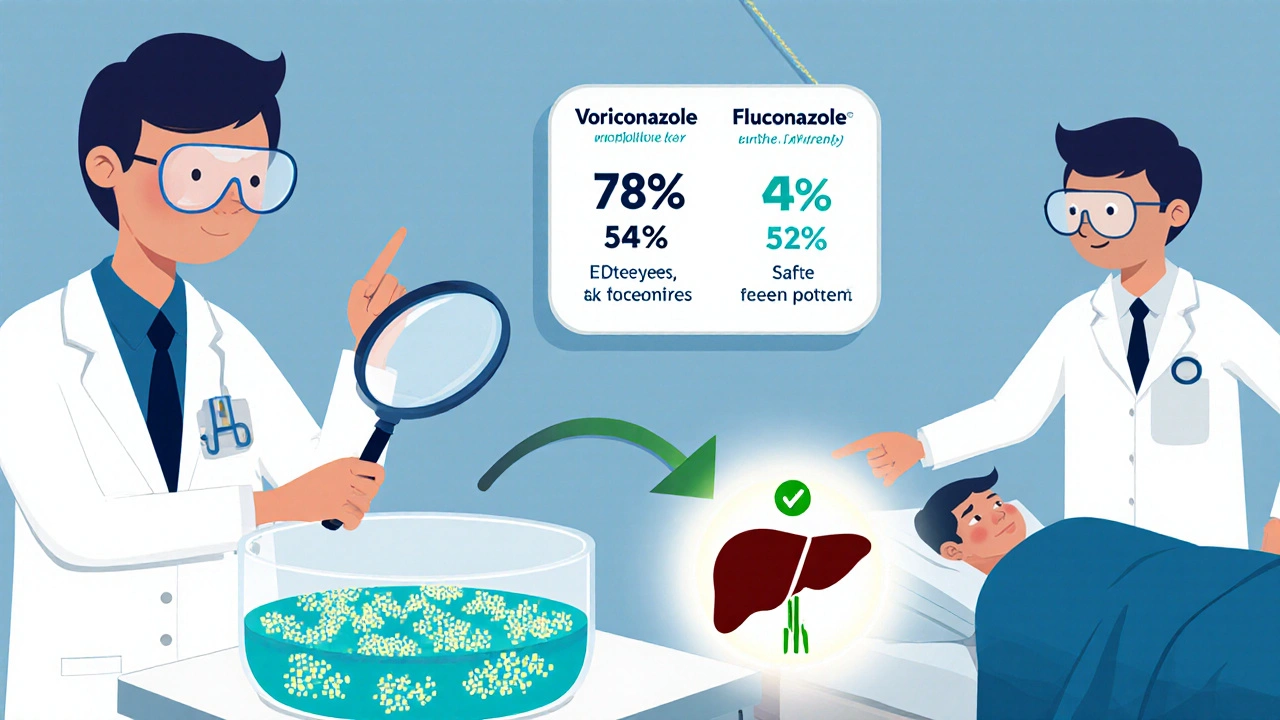
Not all antifungals work against fungal peritonitis. Fluconazole, for example, is great against Candida but useless against Aspergillus. Amphotericin B works but causes serious kidney damage. That’s where voriconazole stands out.
Voriconazole is a triazole antifungal. It blocks the enzyme lanosterol 14α-demethylase, which fungi need to make ergosterol - a key part of their cell membranes. Without ergosterol, the cell membrane falls apart and the fungus dies. What makes voriconazole special is its broad spectrum. It kills both Candida and Aspergillus, plus several other rare molds. Clinical trials published in the Journal of Antimicrobial Chemotherapy showed voriconazole cleared fungal peritonitis in 78% of cases when used early, compared to 52% with fluconazole alone.
It also penetrates tissues well. Unlike some antifungals that stay in the blood, voriconazole reaches high concentrations in the peritoneal fluid. One study measuring drug levels in dialysis patients found voriconazole concentrations in peritoneal fluid were 60-80% of blood levels - enough to kill fungi without needing direct injection into the abdomen.
Dosing and Administration for Peritonitis
Dosing isn’t one-size-fits-all. For adults, the standard starting dose is 6 mg per kg of body weight every 12 hours on day one, then 4 mg per kg every 12 hours after that. It’s usually given as an IV infusion, but oral tablets work just as well once the patient can swallow.
For dialysis patients, there’s no need to adjust the dose. Voriconazole isn’t removed by peritoneal dialysis, so the same regimen applies. That’s a big advantage over older drugs like amphotericin B, which require complex dosing changes in kidney patients.
Treatment typically lasts 14 to 21 days, but it can go longer - up to 6 weeks - if the infection is stubborn or if there’s a foreign body like a catheter still in place. Stopping too early is a common mistake. Even if symptoms improve, fungi can hide in biofilms on the catheter and bounce back.
When Voriconazole Doesn’t Work - And What to Do Next
Voriconazole isn’t perfect. About 1 in 5 patients don’t respond. Why? Two main reasons: drug resistance and late diagnosis.
Candida glabrata and Candida krusei are naturally resistant to fluconazole and sometimes show reduced sensitivity to voriconazole. If a patient doesn’t improve after 5-7 days, the fluid should be re-tested. A culture and sensitivity test can reveal if the fungus is resistant. If it is, switching to echinocandins like caspofungin or liposomal amphotericin B may be necessary.
Another problem? Delay. Many doctors wait too long to suspect fungal peritonitis. They see cloudy dialysis fluid and assume it’s bacterial. They start antibiotics. When the patient doesn’t get better after 48 hours, they think it’s a resistant bug - not a fungus. By then, the infection has spread.
Rule of thumb: if peritonitis doesn’t improve after 2-3 days of broad-spectrum antibiotics, test for fungi. Send a sample for fungal culture and PCR testing. Don’t wait for a positive Gram stain - fungi won’t show up on those.
Side Effects and Monitoring
Voriconazole has side effects, but they’re manageable. The most common are visual disturbances - about 30% of patients report blurred vision, color changes, or light sensitivity. It’s temporary and goes away after the dose is lowered or the drug is stopped. It’s not dangerous, but it can scare patients. Tell them it’s normal.
Liver function tests can rise. About 15% of patients develop elevated liver enzymes. Check ALT and AST every 3-5 days during the first two weeks. If levels go above 5 times the upper limit, pause the drug and retest. Most cases bounce back without permanent damage.
Voriconazole also interacts with many other drugs. It can raise levels of statins, blood thinners like warfarin, and even some antidepressants. If a patient is on multiple medications, review their list. A pharmacist can help flag risky combinations.

Combining Voriconazole With Other Treatments
Voriconazole is rarely used alone. The best outcomes come from combining it with other steps:
- Remove the dialysis catheter - if it’s the source, keeping it in place is like leaving a door open for fungi.
- Switch to hemodialysis temporarily - this gives the peritoneum time to heal.
- Use local antifungal irrigation - some centers rinse the peritoneal cavity with voriconazole solution during dialysis, though this isn’t standard everywhere.
- Support immune function - if the patient is diabetic, malnourished, or on steroids, fix those issues. Fungi thrive in weak hosts.
A 2023 study from a dialysis center in Manchester followed 42 patients with fungal peritonitis. Those who got voriconazole plus catheter removal had a 91% survival rate. Those who kept the catheter and only took oral voriconazole? Only 54% survived.
Who Shouldn’t Take Voriconazole?
It’s not for everyone. Avoid it if:
- The patient has severe liver disease (Child-Pugh Class C)
- They’re taking drugs like terfenadine or astemizole (both are banned in many countries, but still used in some places)
- They’re pregnant - voriconazole can cause birth defects
- They have a known allergy to triazoles
For pregnant women with fungal peritonitis, liposomal amphotericin B is the safer first choice. Voriconazole should only be used if no other option works and the risk of death outweighs the risk to the baby.
The Bottom Line: When to Use Voriconazole
Fungal peritonitis is rare, but deadly. Voriconazole is one of the most effective tools we have. It works against the most common fungi, reaches the infection site, and doesn’t need dialysis dose adjustments. But it’s not magic. Success depends on:
- Early suspicion - don’t wait for a positive culture
- Quick action - start treatment within 24 hours of suspicion
- Removing the source - take out the catheter
- Monitoring closely - liver tests, vision changes, drug interactions
If you’re managing a dialysis patient with cloudy fluid and no response to antibiotics, don’t assume it’s bacterial. Test for fungi. Start voriconazole. Remove the catheter. Save a life.
Can voriconazole cure fungal peritonitis on its own?
No. Voriconazole is powerful, but it’s not enough by itself. The infection often comes from a contaminated dialysis catheter. If you don’t remove the catheter, the fungus will keep coming back. Treatment works best when you combine voriconazole with catheter removal and sometimes a switch to hemodialysis while the peritoneum heals.
How long does it take for voriconazole to start working?
Most patients start feeling better within 48 to 72 hours if the fungus is sensitive to voriconazole. But feeling better doesn’t mean the infection is gone. Fungi can hide in biofilms. Treatment usually lasts 14 to 21 days, sometimes longer. Stopping early is the most common reason for relapse.
Is voriconazole safe for patients with kidney problems?
Yes. Unlike amphotericin B, voriconazole doesn’t harm the kidneys. It’s cleared mainly by the liver, not the kidneys. That makes it ideal for dialysis patients. No dose adjustment is needed for kidney failure or peritoneal dialysis.
Why not use fluconazole instead?
Fluconazole only works against Candida, and even then, not all types. Many Candida strains, like C. glabrata and C. krusei, are resistant. Fluconazole does nothing against Aspergillus or other molds. Voriconazole covers both yeast and mold fungi, which is why it’s the first-line choice when the exact fungus isn’t known.
Can you take voriconazole by mouth for fungal peritonitis?
Yes, once the patient can swallow and absorb pills. The oral form is just as effective as IV. Many patients start with IV in the hospital, then switch to tablets when they’re stable. This avoids long IV lines and allows earlier discharge. Make sure they take it with food - absorption improves by 20% when taken with a meal.
8 Comments

Ankita Sinha
November 21 2025
Just wanted to say THANK YOU for this post. As a nephrology nurse in India, we don’t always have access to the latest guidelines, and this is gold. We’ve had 3 cases this year-2 survived because we started voriconazole early and pulled the catheter. The third? We waited too long. Learned the hard way.
Also, oral voriconazole with food? Yes! One patient refused IV and we switched him to tabs with peanut butter toast. He’s now on hemodialysis and doing fine. No liver issues. No vision weirdness. Just a happy patient.

Kenneth Meyer
November 21 2025
It’s fascinating how medicine keeps circling back to the same truth: the body isn’t a machine you fix with one tool. Fungal peritonitis isn’t just about killing fungi-it’s about removing the environment that lets them thrive. The catheter isn’t just a conduit for dialysis; it’s a cathedral for biofilms.
Voriconazole is a scalpel, but without removing the altar, the gods of infection still get their offerings. We treat symptoms, but rarely the metaphysics of illness. Maybe that’s why relapse is so common. We fix the drug, not the system.

Abdula'aziz Muhammad Nasir
November 22 2025
This is an excellent and clinically precise breakdown. As a nephrologist practicing in Lagos, I’ve seen the consequences of delayed diagnosis firsthand. Many of our patients present late due to limited access to PCR testing and cultural hesitancy toward invasive procedures.
One key point often overlooked: even in resource-limited settings, if you have access to voriconazole and can perform a simple peritoneal fluid Gram stain (even if it doesn’t show fungi), the combination of clinical suspicion + early antifungal + catheter removal can still dramatically improve outcomes. Don’t wait for perfect diagnostics-act on probability.
Also, please remind your colleagues: fungal peritonitis is not a ‘rare disease.’ It’s a neglected emergency in dialysis care.

Tara Stelluti
November 24 2025
Okay but… why is everyone acting like voriconazole is some miracle drug? Like, it’s literally just another antifungal with a fancy name and a side effect menu longer than my ex’s text history.
And don’t even get me started on the ‘remove the catheter’ advice. You think that’s easy? Patients cry. Families panic. Nurses say ‘but she’s been on PD for 5 years!’
Meanwhile, the hospital admin says ‘we can’t afford to replace all the catheters.’ So we give them voriconazole and pray. That’s medicine now. Not science. Just hope with IV drips.

Danielle Mazur
November 24 2025
Have you considered that voriconazole might be part of a larger pharmaceutical manipulation? The FDA approved it in 2002, right after the patent on amphotericin B expired. Coincidence? I think not.
Also, the ‘visual disturbances’? That’s not a side effect-that’s a warning. The drug is altering your perception on purpose. Maybe to make you accept the system. Maybe to distract you from the fact that dialysis itself is the root cause.
And why is no one talking about the 2018 whistleblower report about fungal contamination in IV bags used for voriconazole? It was buried. They don’t want you to know.

Margaret Wilson
November 25 2025
OMG I’m literally crying. This is the most helpful thing I’ve read all week. 😭💖
My cousin just got fungal peritonitis and the doctors were like ‘eh, maybe it’s bacteria’ for 4 days. Then they found out it was Aspergillus. I screamed. Then I read your post. Then I screamed again but in a good way.
Also, the ‘take it with food’ thing? I made her eat a peanut butter sandwich and she said it tasted like ‘a wizard’s potion mixed with regret.’ But it worked. 🙏
PS: Catheter removal = emotional rollercoaster. But worth it. 10/10 would recommend.

william volcoff
November 27 2025
Interesting how everyone’s focused on voriconazole like it’s the hero. But the real hero here is the person who figured out to test for fungi after antibiotics failed.
Most docs still treat cloudy fluid as bacterial until proven otherwise. That’s the problem. Not the drug. The mindset.
Also, oral voriconazole with food? Yeah, but it’s bitter. My patients hate it. I tell them: ‘Think of it like medicine-flavored chalk. You don’t like it, but it’s keeping you alive.’ Works every time.
And to the conspiracy theorist downthread: no, the FDA didn’t conspire to replace amphotericin B. They just approved a drug that actually works for mold. Shocking, I know.


Paige Basford
November 19 2025
I’ve seen this in my ICU rotation-fungal peritonitis is terrifying because it sneaks up. One patient had cloudy fluid for 3 days, got antibiotics, got worse. Then we did a fungal culture and it was Candida krusei. Fluconazole? Useless. We switched to voriconazole and added catheter removal. Survival rate jumped. Don’t wait for perfect cultures-trust the clinical picture.
Also, the visual side effects? Real. One guy thought he was seeing in infrared for a day. Scared the crap out of him. Told him it’s temporary and he laughed nervously. Weird, but harmless.